COMMON FOOT AND ANKLE INJURIES IN DANCE
By: Robert H. Sheinberg, D.P.M., D.A.B.F.A.S., F.A.C.F.A.S.
CAUSES OF INJURIES:
Overuse injuries are common due to the repetitive nature of dancing. They most commonly involve the tendons around the back and inside of the ankle. These injuries are more common in dancers who do not properly stretch or increase training time too rapidly in preparation for a performance.
Mishaps may occur from stepping incorrectly or landing from a jump. They most commonly involve the ligaments on the outside of the ankle.
Technical Errors occur when dancers are improperly trained. Proper technique is critical as a way of preventing injury.
Physique, because of the special requirements of certain types of dance, some body types are predisposed to recurrent injuries.
INJURY TYPES:
1. Achilles Tendon – Injuries to the Achilles tendon are usually due to inflexibility of the calf muscles and overuse of the tendon. They are more common in dancers who are flatfooted and go barefoot. Stiffness and soreness are usually felt after getting up from sitting and starting to walk. The pain usually lessens or even goes away with activity but recurs later. Rest, ice and physical therapy may be necessary to allow the inflammation to recede. Wearing a shoe with a small heel when not dancing may be indispensable in resting the tendon after it has been used. When the injury has not improved a short period of immobilization in a removable boot may be necessary to allow the area to heal. In some cases the dancer can continue to perform but as soon as the performance is done the removable boot is reapplied so that it rests the remainder of the day. The boot or a night splint may also be necessary to improve the flexibility of the calf. If the condition advances and causes discomfort throughout the day, immobilization in a fiberglass cast may be needed to completely rest and allow the area to heal.


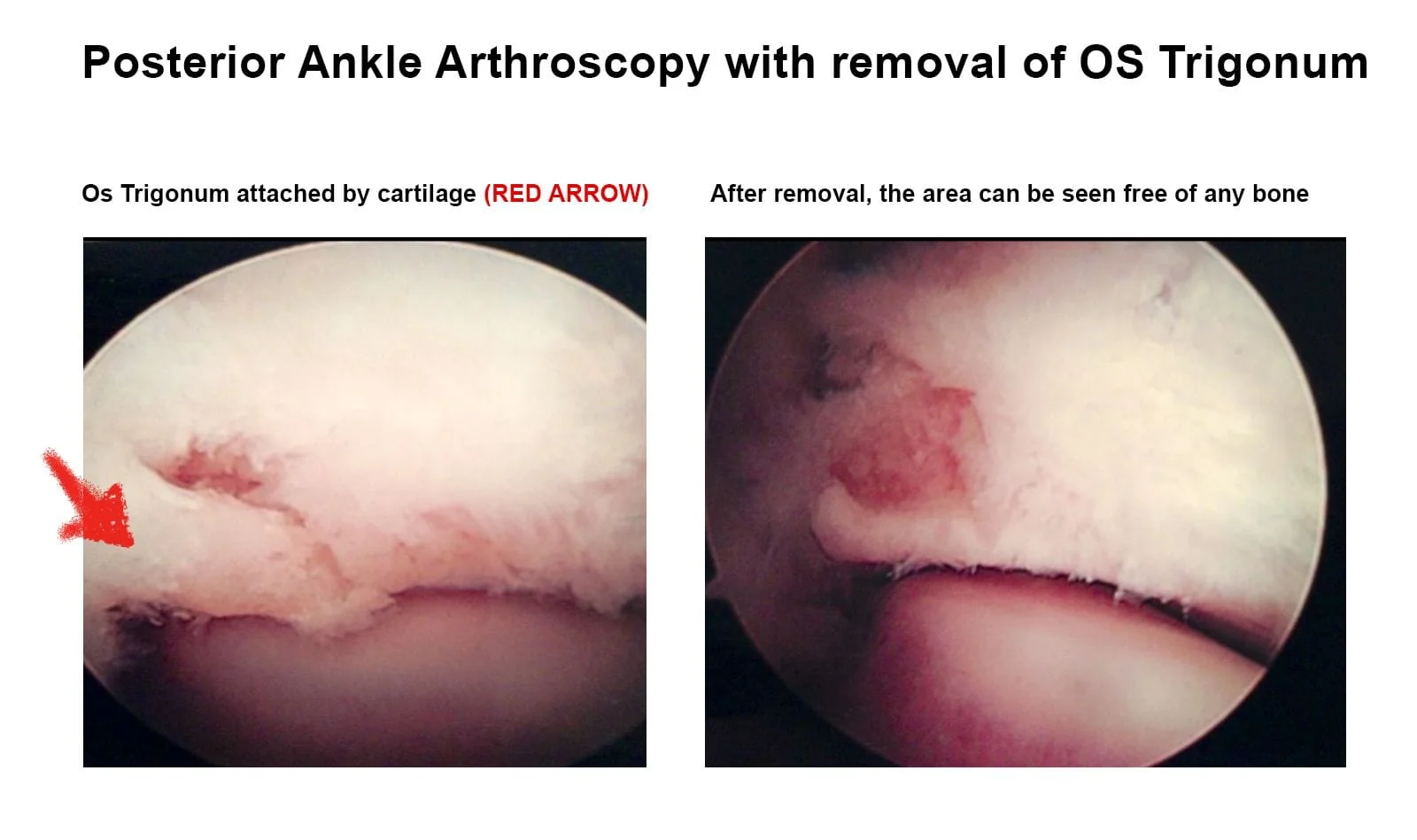
2. Impingement Syndrome - Pain in the front or back of the ankle can occur from a dancer standing “on point” or “demi point”. The pain in the back of the ankle is made worse by the foot pointing down and may be caused by a small fracture to the cartilage in the back of the ankle (os trigonum). An injury to this area may require a period of immobilization to allow the area to heal. In some cases this can become a recurrent problem and a small piece of bone may be removed to allow the dancer to return to full activity.



Pain in the front of the ankle is usually caused by thickening of the ankle joint lining and can cause pain while moving the leg forward on the foot. This impingement syndrome is usually associated with an ankle ligament injury and can become very painful, especially the first thing in the morning when getting out of bed to walk or after sitting for a short period of time and getting up to walk. The inflammation and soreness usually lessen with activity but return later on in the day. Physical therapy and a short course of anti-inflammatory medication may be necessary to reduce the inflammation in the ankle joint. If that does not improve, a cortisone injection may be necessary to reduce the thickening of the soft tissue. In some cases the impingement in the front part of the ankle does not improve and arthroscopic debridement may be necessary to completely regain the ankle mobility without discomfort. In some cases a small spur is present on the front part of the lower leg bone. This can cause chronic pain and stiffness in the ankle. If present, arthroscopic removal of the bone spur is also performed to allow the dancer to resume activity.
3. Stress Fractures - Stress fractures are microfractures that usually occur in the front part of the shin bone (tibia), the outer leg bone (fibula) or the top of the foot (metatarsal). The most common presentation is a dancer who presents with a sudden alteration in their training regimen (increased training intensity) that develops pinpoint pain and localized swelling over the bone. This type of injury is more common in teenage girls, especially those with menstrual irregularities and lower calcium intake. Treatment includes immobilization in a walking boot for 4-8 weeks to allow the bone to heal. Depending on the degree of injury to the area some dancing may be allowed during the healing process.
4. Sprained Ankle - The most common traumatic injury in dance is a twisting injury to the ankle that disrupts the ligaments on the outside of the ankle. Pain, swelling and discoloration may occur and is proportional to the magnitude of the injury. Difficulty weightbearing may be a sign that the ligament(s) may be torn. Immediate treatment includes temporary immobilization in brace or cast to minimize damage. Physical therapy begins once the injury stabilizes. In some cases inflammation of the joint causing an impingement syndrome prevents the dancer from returning to full activity. When conservative care fails to alleviate the pain, arthroscopic removal of the soft tissue that is causing the impingement will allow the dancer to return to activity very quickly. Occasionally, chronic instability may develop causing the ankle to twist very easily with activity. If the physical therapy does not improve the ankle’s strength and mobility, tightening the ligaments on the outside of the ankle surgically followed by a short period of immobilization and physical therapy will allow the dancer to resume all activities without any problems.
5. Sesamoid Injuries – Sesamoids are bones the size of a pea on the ball of the foot just under the big toe joint. Frequent jumping on the ball of the foot may cause the bone to break or injure the cartilage that covers it. These injuries are very painful and do not allow dance participation. Tenderness is directly on the bone on the ball of the foot. Treatment includes immediate rest and immobilization of the foot to allow it to heal. Cast and often crutches are needed to give it the rest necessary to allow complete resolution of the symptoms. Following immobilization orthotics are used to unload the sesamoids. Surgery, although rarely necessary, may be needed to resolve the condition if conservative treatment fails. In most cases this will allow the dancer to resume activities without any long-term problems.

6. Bunions – A prominence of bone on the inside of the foot is called a bunion. This is not a growth of bone but shifting of the bones in the foot that is starting to take place. This is a hereditary condition that is made worse by dancing. Dancing will not cause bunions. Nonpainful bunions do not require any treatment. Unfortunately, bunions are progressive and the condition gets worse over time. In addition, arthritis does develop in the big toe joint, causing problems in the future. If the bunions are painful the patient may need surgery to correct the problem. This will allow complete future participation and dance without any problem. The old thoughts of not operating on dancers does not hold true any longer. Advance techniques allow complete restoration of joint movement and prevention of arthritis years later.


7. Hallux Rigidus – Early arthritic changes may develop in the big toe joint, limiting joint mobility. Structural problems of the foot or an injury to the big toe joint may set up a cascade of events that will limit the joint’s ability to move. Bone spurs may develop on the top of the big toe joint, limiting the ability of the big toe to move up. Joint stiffness and soreness is usually present, especially when “on point”. Early aggressive treatment with physical therapy and orthotics may be needed to lessen the inflammation and improve the joint’s mobility. In most cases surgery is needed to improve the joint’s flexibility. Unfortunately, conservative care only helps for a short period of time. Cortisone injections should not be given in the big toe joint, as this will cause further degeneration of the cartilage.

8. Heel Pain – Heel pain in dancers is common, especially in the 8 to 14-year-old age group. Tight calf muscles and dancers that are flatfooted contribute to this problem. It is also commonly seen during growth spurts. Symptoms include mild discomfort in the heel towards the end of an activity. Occasionally stiffness in the foot and ankle in the morning may be present. Tenderness is felt in the back of the heel with touching or grasping of the heel bone. No associated discoloration or swelling are ever seen. If swelling is present a stress fracture may have developed to the heel bone. Treatment includes Taping the foot to support the heel and prevent pulling of the Achilles tendon and plantar fascia on the heel bone. Proper shoe gear while the dancer is not performing is also necessary to lessen some of the stress to the area. A shoe with a small heel is ideal. It is necessary for the dancer to avoid going barefoot at all times. Heel lifts in sneakers and orthotics may permanently alleviate the pain. Physical therapy may be necessary to improve overall muscle flexibility. If unresponsive to this conservative treatment approach immobilization in a cast or a brace may be necessary to completely rest the area and allow the dancer to heal completely and resume all activity.



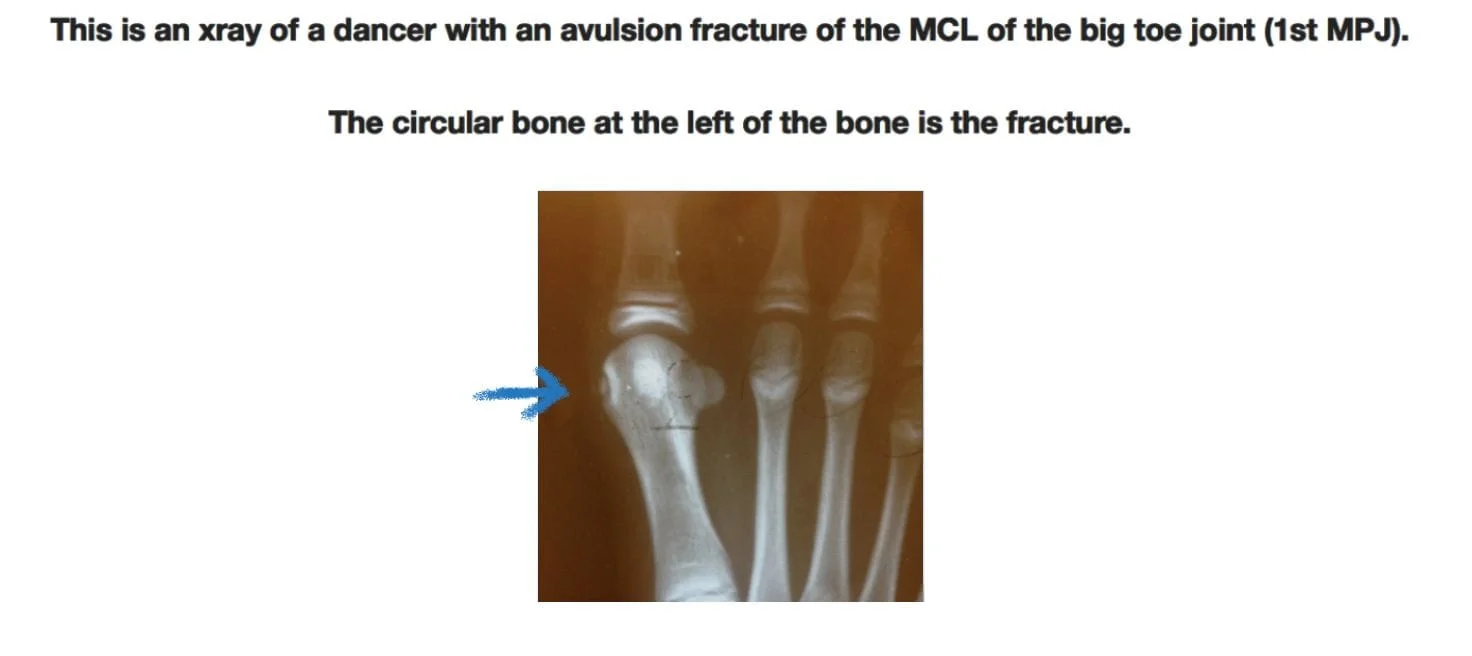
9. Trauma (other) – Avulsion fractures from sprains of joints and ligaments, Muscle tendon tears
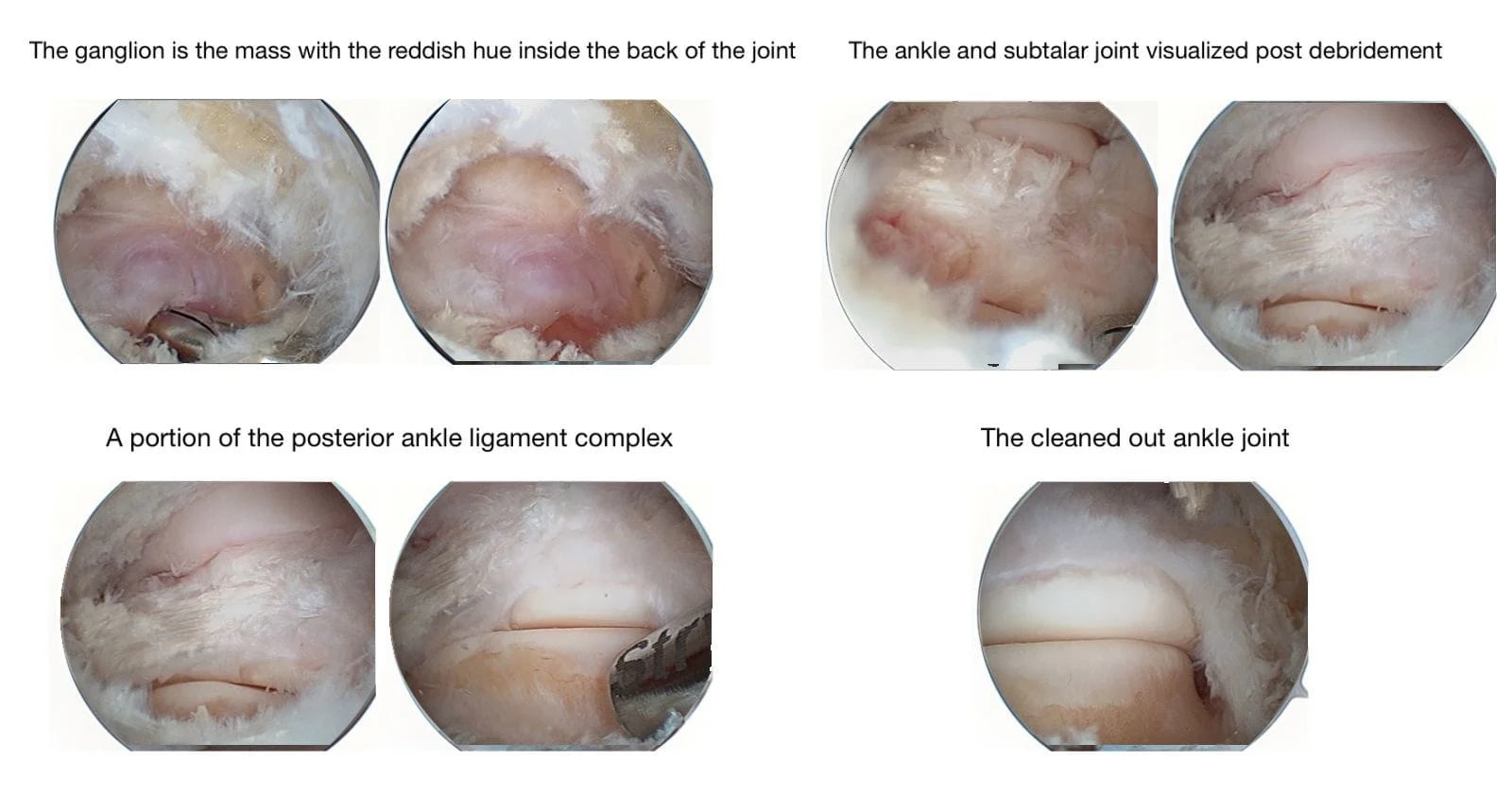
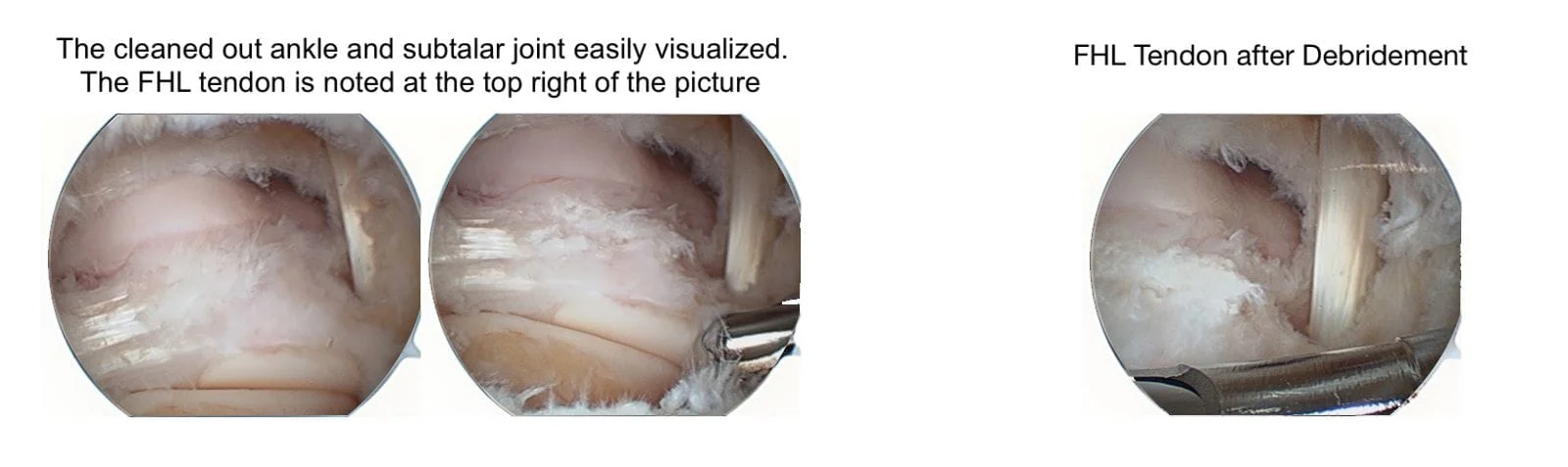
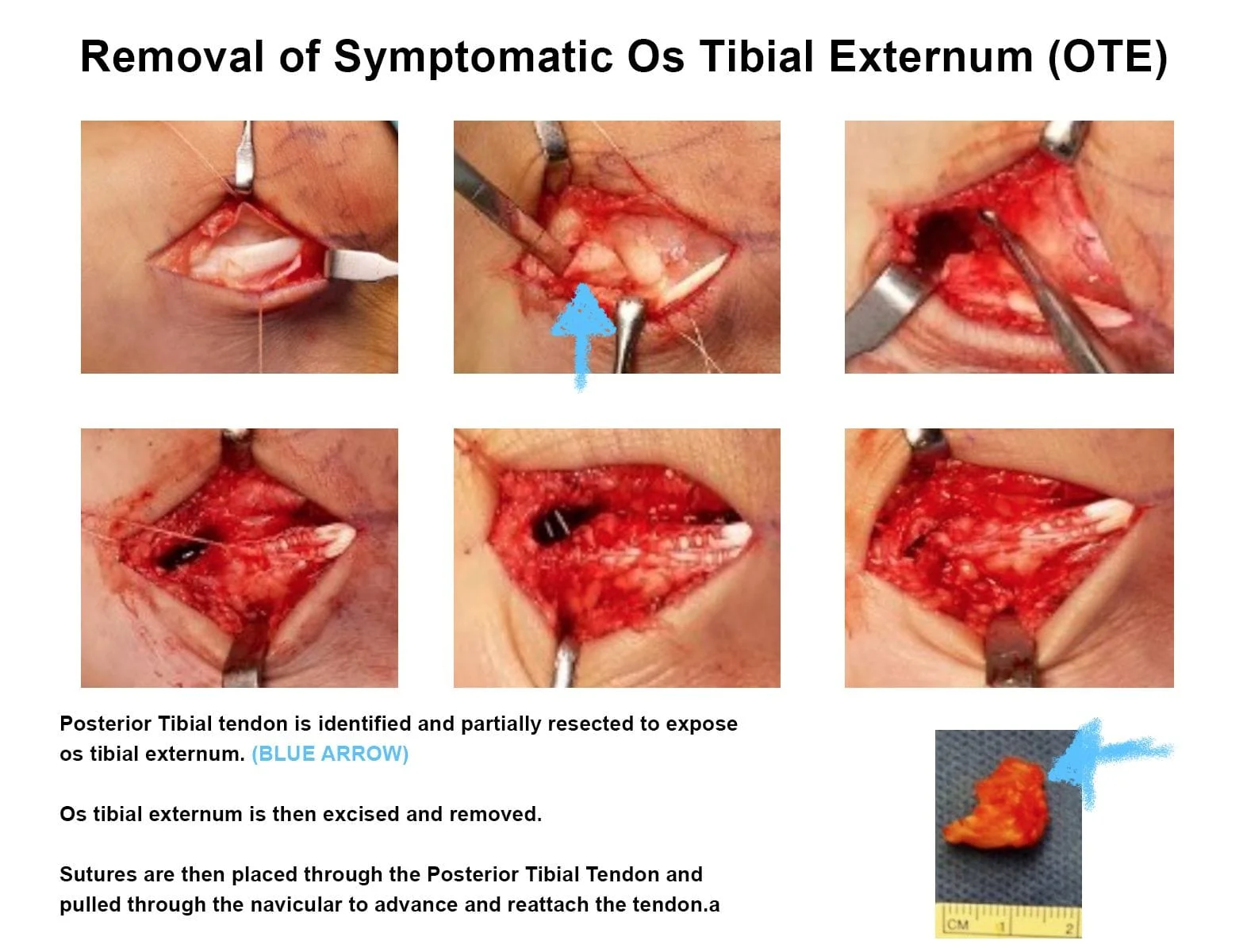
SURGICAL PICTURES

Posterior Ankle Arthroscopy with removal ganglion cysts