GENU VALGUM (KNOCK-KNEE)
By: Robert H. Sheinberg, D.P.M., D.A.B.F.A.S., F.A.C.F.A.S.

What is Genu valgum?
Genu valgum is a normal developmental variation. At birth, the knee is
usually in a bowlegged posture (genu varum). By age 2 the angle of the upper
leg bone relative to the lower leg bone starts to straighten. The knee then
goes into a knock-kneed posture progressively until it maximizes at
approximately age 4. The knock-kneed appearance then lessens into a more
adult value by age 10-12.
How is it evaluated?
The distance between the bones on the inside of the ankle is measured
(intermalleolar distance). At age one the distance between the inner aspects
of the knees is approximately 0 and the distance between the inner ankle
bones (intermalleolar distance) is approximately 2 cm. By age 3-4 it is
approximately 4 cm and slightly decreases into adulthood. X-rays may also be
taken of the entire lower extremity and the angle made of the upper leg bone
relative to the lower leg bone is evaluated. At birth, the angle is towards
a bowlegged appearance. The angle approaches neutral (0 degrees) by
approximately age 2. By age 3-4 it is approximately 4 cm, slightly decreases
into adulthood. If intermalleolar distance can be considered within normal
limits up to 8 cm between the ages of 2 and 11.
What kind of symptoms are associated with genu valgum?
Genu valgum is often associated with a flatfoot deformity. When the knees
are in an excessive knock-kneed posture the joints in the foot (subtalar
joint) have to rotate out. This puts excessive stress and strain on the
ligaments, tendons and soft tissue in the inner arch and ankle area.
Children that are excessively knock-kneed and flatfooted run very poorly and
generally lack coordination relative to their peers. They fatigue
prematurely with activity and do not participate in sports at the level of
their peers. Knee problems are very common in children that are knock-kneed.
Malalignment of the patellofemoral joint is commonly seen, creating an
imbalance. Abnormal tracking of the patella (kneecap) in its groove may
predispose it to chondromalacia, patellar subluxation. Also associated with
excessive knock-knee is excess stress to the inner aspect of the upper and
lower leg bone (medial tibial stress syndrome). This is commonly referred to
as shin splints. As an adult, excessive knock-knees are associated with
premature wear of the cartilage on the outside of the knee joint, causing
arthritis to take place.
What types of treatment are indicated for my child?
Evaluation of the entire lower extremity is important. Any associated
problems including flatfeet must be addressed. Flatfeet can be addressed by
placing an orthotic in a shoe. This will prevent the arch from increased
stress and the potential for further breakdown. It would also help the
child’s gait improve and lessen the fatigue that may be associated with the
deformity. An overweight child can also attempt to lose weight to unload the
knee. It is best to place him on exercises that do not stress the knee.
Swimming and cycling seem to be best. Bracing of the knee may provide some
benefit, especially if the knee clinically and the angles seen on x-ray
appear to be abnormally high.
What other conditions must be ruled out in my child with excessive
knock-knee?
Some conditions may predispose a child to be knock-kneed. The most common is
a fracture that occurred in the upper portion of the lower leg bone
(proximal metaphysical tibial fracture). This has a tendency to allow the
leg to drift into a valgus posture. Metabolic disturbances (hypophosphatemic
rickets), multiple epiphyseal dysplasia and pseudoachondroplasia must also
be ruled out via x-rays.
Can surgery be performed?
Correction of the deformity may be indicated in certain children. Gait
disturbances, foot, ankle, leg and knee discomfort, gross patella
malalignment and evidence of ligamentous laxity in the knee or cosmetic
concerns collectively may indicate the need for surgical correction of the
deformity. It should be delayed until after the age of 8-10, depending on
the degree of deformity.
Below is an x-ray image of genu (knee) valgum where the femurs above the knee and tibia-fibula below the knee are angling away from the midline of the body.

Pics below of Knock knee pediatric girl. Due to the angulation of the legs, the feet pronate in even more as can be seen in the bottom pic.



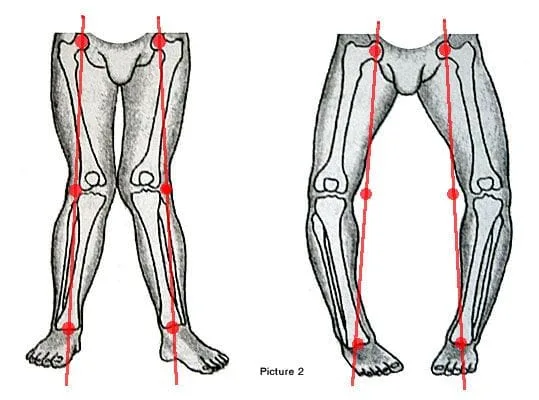
Below is an illustration comparing genu valgum (knock knee) on the left to genu varum (bowleg) on the right.