PERONEAL TENDONS
By: Robert H. Sheinberg, D.P.M., D.A.B.P.S., F.A.C.F.A.S.
The peroneal tendons are two strong tendons that connect the muscles on the outside of the leg to the bones in the foot. They run behind the bone in the ankle called the fibula. When they contract they move the foot down and out. They play an important role in stabilizing the foot on uneven surfaces. When the foot turns excessively in (i.e. attempt at ankle sprain) these tendons contract and stabilize the ankle so that it does not twist too far in. Tendons are covered by a ligament called the peroneal retinaculum. It is a strong ligament that connects the outer leg bone (fibula) to the heel (calcaneus). The ligament covers the peroneal tendons and helps keep them in a groove behind the fibula. Under normal circumstances it helps to allow the tendons to contract with extremely high forces without dislocating. Without this ligament restraint, the muscle tendon unit cannot generate enough force during activity. If the tendons dislocate, they do not have a normal mechanical advantage and they become weak and painful and tears often develop in the tendon.
CAUSE:
- Weak or loose ligament that covers the tendons can allow the tendons to dislocate.
- A shallow groove in the fibula may not allow the tendons to seat properly.
- Twisting injury to the ankle that causes the tendons to over contract and tear the ligament that covers it.
- Twisting injury to the ankle may cause a severe contraction causing a fracture off of the fibula, allowing the tendons to dislocate.
- Anomalous muscle in the outer part of the ankle.
- Hypertrophy of a normal muscle causing too much bulk on the outside of the ankle.

SIGNS AND SYMPTOMS:
- Swelling behind the fibula on the outside of the ankle.
- Popping sensation with movement of the foot down and in and up and out.
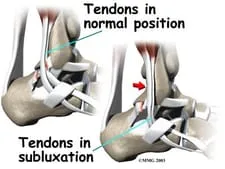
- Appearance of the tendons in the front part of the ankle instead of in their normal position behind the fibula where they are not visible.
- Weakness with activity.
- Frequent ankle sprains.
- Often associated with a tear of the peroneus brevis tendon.
- May be associated with ankle ligament injury and chronic instability of the ligaments in the ankle.
TREATMENT:
- X-rays are usually taken to see if any bone injury has occurred in conjunction with the ligament tear.
- MRIs are necessary to evaluate not only the injury to the ligament but also the tendon to identify any split tears. CT scans may be necessary to evaluate the depth of the groove in the fibula. When shallow, flat or convex it may be necessary to repair this at the same time.
- If an acute injury is seen early, immediate application of a cast will possibly allow the ligament to heal while keeping the tendons in their proper place behind the fibula.
- If unresponsive to casting, surgical repair of the ligament is necessary.
- If a shallow groove in the bone is seen it may be deepened to allow the tendon to sit in a better position without recurring subluxation.
- If a tendon is also torn it is repaired at the same time as the ligament that holds it in place.
- If chronic instability of the ligaments in the front of the ankle is seen at the same time they are also repaired to allow more normal ankle function and a full return to activity.
- Any anatomical variant is addressed at the time of surgery, including removal of any anomalous muscle that may be contributing to the recurrent subluxation.
PROGNOSIS:
- Excellent in a recreational or professional athlete allowing future participation at the preinjury level.
***********
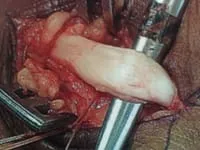
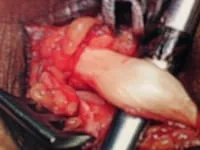
Below, Peroneal Tendon Tear with low-lying muscle belly that is being removed in 3rd pic. The tendon is then repaired and tubularized.




Below, Peroneal Tear with Low lying muscle belly. The muscle belly is removed and ebulked to allow gliding and reduce congestion.



The muscle belly is seen at the right and closure of the sheath on the left and bottom pics.



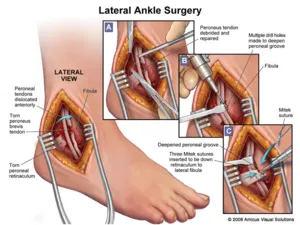
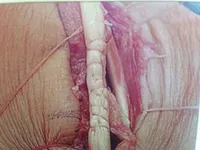
Below, dislocated peroneal tendons are being repaired and reduced to the anatomic location.
The tendons are dislocated to the outside of the fibula instead of behind.


This is a pic of us relocating the tendons.

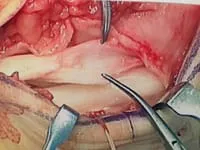
The following pic is of us debriding the side of the fibula to allow the ligament and tissue to connect to the fibula during healing so the tendons do not dislocate.

This is a pic of the suture passing through the fibula to attach the retinaculum and tissue so the peroneal tendons do not dislocate or sublux.

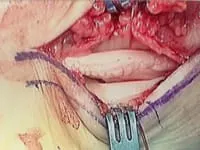
This is a final pic of the repair

Pics of repair of peroneal retinaculum for dislocating peroneal tendons
The sutures can be seen prior to repair


The retinaculum is repaired through drill holes in the fibula and the sutures are woven through the bone

Pic after complete repair

Split Tear of the Peroneus Brevis.
The torn damaged portion is removed and the tendon is repaired onto itself


Intrasubstance tear with bulbous thickening before and after repair


Bulbous thickening of peroneus brevis with split thickness tear



The bulbous portion is removed and the remainder of the tendon is repaired back onto intself.



Split thickness tear before and after excision of portion of tear


Flattening of Peroneus Brevis before and after repair


Split tear of peroneus brevis before and after repair
Bulbous thickening of the Peroneal tendon

The tear inside the bulbous thickening is resected and the tendon is repaired onto itself


Pics of intrasubstance tear of peroneus longus


Pic after removal of diseased portiom

After closure of the tendon sheath

Pic split tear of Peroneus longus


Pic of low lying muscle belly of peroneus longus causing pain

Split tear of Peroneus longus prior to repair


After suture repair

Pic of intrasubstance tear of peroneus longus


Pic during excision of diseased tendon

Pic after repair

Pic of Split tear of the Peroneus Brevis and section that was removed. This is caused by the Peroneus longus constantly pushing the Brevis into the back of the fibula. It can be due to repeated microtrauma or one isolated traumatic event, i.e. ankle sprain or fracture).



Pic of Split tear of the Peroneus Brevis and section that was removed. This is caused by the Peroneus longus constantly pushing the Brevis into the back of the fibula. There was also a low lying muscle belly of the Brevis that was removed with the damaged tendon. This can be seen at the left side of the removed tendon. The tear can be due to repeated microtrauma or one isolated traumatic event, i.e. ankle sprain or fracture).



